
Age
Participants were asked to provide their age. Most participants were between ages of 18 and 45. Figure 1 depicts participants’ age at the time they took the survey.

Figure 1: Participants’ age distribution.
Age of onset of keloid disorder
Participants were also asked to record the age they developed their first keloid lesion. Peak age of onset among all participants was 16, with most developing their first keloid between the ages of 5 and 25. Figure 2 depicts participants’ reported age at the time they developed their first keloid lesion.

Figure 2: Age of onset of keloid disorder among the study population.
Country of Birth
A total of 190 participants provided information about their country of birth. Most (57.9%) were born in the United States, 5.8% were born in India, 3.2% were born in United Kingdom, 3.2% were born in Canada, and 2.6% were born in Philippines. Figure 3 depicts the country of birth for all study participants.
Although this distribution pattern correctly represents the country of birth of those who participated in this study, it is by no means a true reflection of the epidemiology of keloid disorder and is most likely a reflection of the level of healthcare services that might have been available to the patients. Furthermore, this information does not take into consideration the migration patterns or the patients’ country of residence.

Figure 3: Country of birth of the study participants.
Ethnicity
Participants were asked to provide their ethnic background. A total of 190 participants provided this information. Figure 4 shows percentages for different ethnic characteristics. Although this information is a correct representation of those who participated in this study, it is not a true reflection of the ethnic epidemiology of keloid disorder.

Figure 4: Participants’ ethnic background.
Pattern of Distribution of Keloid Lesions
Participants were asked to provide detailed information about the distribution of keloid lesions throughout their skin. Chest, shoulders, ears, and upper arms were the most frequently involved areas. Figure 5 depicts the distribution patterns of keloid lesions among the study participants.

Figure 5: Location of keloids. Participants were asked to choose all answers that applied to them.
Appearance and Shape of Keloid Lesions
Participants were asked to describe the shape and the appearance of their keloid lesions. To facilitate their answers, a reference image guide was provided online. As shown in Figure 6, nodular, linear, and flat keloids were the most common forms of keloidal lesions. Among participants, 26.6% considered their keloids to be massive, with keloid lesions occupying large areas of their skin.

Figure 6: Shape of keloid lesions. Participants were asked to choose all answers that applied to them.
Size of keloid lesions:
Participants were asked to describe the size of their individual keloid lesions on their skin. To facilitate their description, a comparison reference guide was provided on the questionnaire. Figure 7 depicts the distribution patterns of the size of keloid lesions.

Figure 7: Size of keloid lesions. Participants with several keloid lesions were asked to choose all answers that applied to them.
Triggering factors
Participants were asked to provide information about the factors that triggered their keloid formation, with 178 providing answers. Figure 8 shows the frequency of various triggering factors within the study population. Acne was by far the most common triggering factor, followed by skin injury and surgery. Fifteen percent of participants listed vaccinations and 13% listed chicken pox as the triggering factor in their keloid development.

Figure 8: Triggering factors. Participants were asked to choose all answers that applied to them.

Figure 9: Number of laser treatments.

Figure 10: Frequency of laser treatments.
When asked about response to treatment, only 4% of participants reported complete resolution of their keloid lesions with laser treatment.;10% reported significant improvement in the appearance of their keloids; 32% reported slight improvement; and most importantly, 54% reported no response to laser treatment. Figure 11 shows the reported response rates to the laser treatments.

Figure 11: Reported response rates to laser treatment.
When asked about the benefit derived from laser treatment, only 3% of participants equated their benefit to cure of their keloid lesions; 27% reported that laser treatment improved their keloids; 47% reported no improvement; and 23% reported that laser treatments actually made their keloids worse.
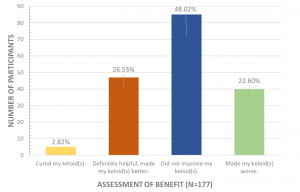
Figure 12: Participants’ assessment the benefits of keloid treatment.
Durability of Treatment Results
When asked about durability of laser treatment, of the 176 participants who provided an answer to this question, 10% reported permanent and durable benefit, 6% reported durability of more than one year prior to recurrence of the treated keloid lesion(s). Figure 13 depicts the durability data collected from participants.

Figure 13: Participants’ assessment of durability of treatment.
FACTORS DETERMINING THE RESPONSE RATES
Various dataset comparisons were performed to identify factors that could have contributed to the response to laser treatments. Comparisons were made between the group who reported responding to laser treatment and those who either reported no response to the treatment or a worsening of their keloids after laser treatment. Participants’ age, age of onset of keloid disorder, number of laser treatments, and shape and size of keloids did not appear to correlate to response to treatment. This analysis only suggested a negative correlation between acne as a triggering factor for development of keloid lesions and the response rate to laser treatment.

Figure 14: Analysis of triggering factors and the response rate to laser treatment between two groups, those who reported responding to treatment and those reported no response to treatment.