
Table 1. Demographics of patients and morphology of neck keloids.
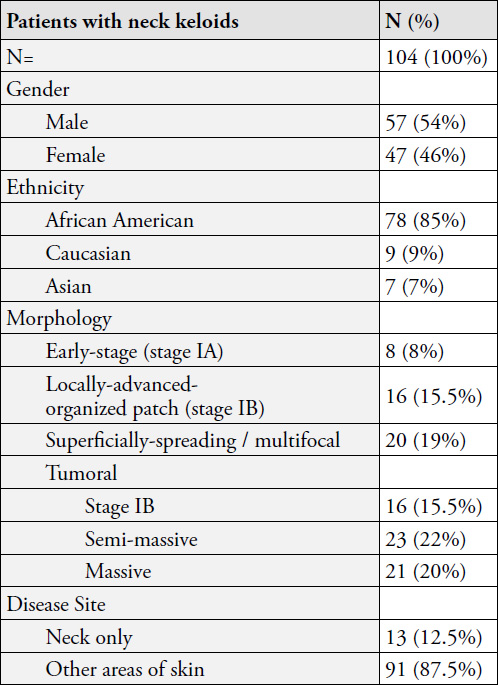

Figure 1. Early-stage papule keloid in a 32-year-old African American female with a 10-year history of keloid disorder, involving her chest and shoulders as well.

Figure 2. Early-stage linear neck keloid in a young Asian male. This lesion was triggered by surgical removal of a mole. A keloid formed at the site of mole removal surgery. The keloid was then excised and the surgical wound was treated with ILT, yet the lesion shown here evolved despite adjuvant interventions. This patient had no other keloids.

Figure 3. Early-stage nodular neck keloid (3a) in a 24-year-old African American male with a four-year history of keloid disorder also involving his face, anterior neck, ears, and chest. This lesion was treated twice with cryotherapy. Figure 3b was taken two years after treatment, showing minimal skin scarring at the site of the treated keloid.

Figure 4. Thick linear keloid of neck in a an African American female.

Figure 5. Case Study 1 – A 55-year-old African American female with a 3-centimeter tumoral keloid in anterior neck.

Figure 6. Case Study 1 – Neck keloid immedicably after application of topical cryotherapy (left, the frozen keloid appears white) and six months later (right) after three cycles of cryotherapy.

Figure 7. Four examples of locally advanced neck keloids. Treating each one of these patients will require a thoughtfully designed long-term plan of care.
Table 2. Subtypes of tumoral neck keloids
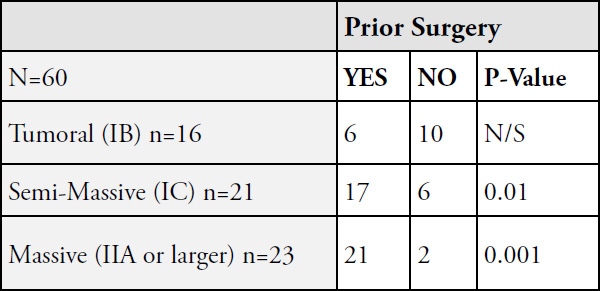
N/S: Not significant
Tumoral neck keloids are almost exclusively seen among African Americans. Among 60 patients with tumoral neck keloids, only three (5%) were non-African American.
Most patients with tumoral keloids have a history of keloid removal surgery. The injury from surgery to either remove a small neck keloid or another pathology is what triggers the formation of tumoral keloids. Therapeutic interventions shall aim at preventing tumoral keloids by avoiding surgery in management of early-stage neck keloids.
Treatment
Cryotherapy is the treatment of choice for all tumoral neck keloids. Surprisingly, these tumors respond well to cryotherapy and can be significantly debulked with one or two courses of cryotherapy. Most patients, however, will need ongoing care and continued treatment to keep the treated keloid under control. ILT and ILC shall be incorporated in management of residual keloid in the base of the debulked keloid.

Figure 8. A 3-centimeter tumoral keloid in anterior neck (left). Significant debulking was achieved after one application of cryotherapy (right, three months later).

Figure 9. A 21-year-old male who presented with a 2 cm anterior neck keloid tumor in May 2011 (9a). The tumor was treated with contact cryotherapy in the same session (9b). Significant debulking was achieved by October 2011 (9c) with cryotherapy alone. Figure 9d depicts durable remission in June 2014.

Figure 10. A 47-year-old male with semi-massive neck keloid that had grown after surgical removal of a smaller keloid.

Figure 11. Same patient as in Figure 10 immediately after application of contact cryotherapy (left – the frozen keloid appears white). Significant debulking was achieved within seven weeks of cryotherapy (right). The remnant of this keloid obviously needs further treatments to achieve better results.

Figure 12. Case Study 2, massive neck keloids at presentation (May 2014). Loss of pigment on the surface of the keloids was secondary to the previously performed spray cryotherapy.

Figure 13. Case Study 2, significant debulking after one course of contact cryotherapy.

Figure 14. Case Study 2, same patient, January 2016. Recurrent disease after cryotherapy.

Figure 15. Case Study 2, noticeable debulking was achieved with repeat cryotherapy (April 2016).

Figure 16. Case Study 2, recurrent disease after repeat surgery and radiation therapy (January 2018).

Figure 17. Case Study 2, debulking achieved with cryotherapy (March 2018)

Figure 18. Recurrent tumoral neck keloid after two previous surgeries in a 42-year-old African American male.

Figure 19. Recurrence of a neck keloid after surgery in a 19-year-old African American female with extensive keloids involving her ears, neck, and pubic areas. She has been struggling with keloid disorder since she was one year old and has undergone numeorus surgeries to remove several of her keloids, with most worse after surgery.

Figure 20. Case Study 3, massive neck keloids in a 25-year-old African American male.

Figure 21. Case Study 3, multiple nodular keloids in submental area three years prior to current presentation and shortly before undergoing the first surgical excision.

Figure 22. Case study 4, a 36-year-old old African American female with massive neck and chest keloids. Note that the neck keloid has merged with the superficially-spreading keloid on her chest.
Case Study 5
A 31-year-old African American male presented in May 2011 with a super-massive keloid tumor involving much of his submandibular neck skin (Figure 23). His struggles with keloid disorder started when he was only 10 years old when he first noticed a minor bump under his jaw. Over the years his disease had progressed and he had been treated with all available modalities, including five surgeries to remove his neck keloid.
All previous surgeries resulted in the worsening and progression of his disease. The last surgery was performed in 2004, and was followed with adjuvant radiation therapy. Due to the size of his neck keloid, the post resection submandibular skin defect had to be closed using a skin graft. This attempt led to the development a new keloid at the donor site on his thigh, an iatrogenic keloid (Figure 23). After all these efforts, this young man simply gave up on all further treatment.

Figure 23. Case study 5, a 31-year-old African American male with super-massive neck keloid and an iatrogenic thigh keloid that developed at the site of donor skin for the skin graft taken to cover the surgical defect created in his neck.
Unfortunately, he is not the only patient who has fallen into this vicious cycle of surgery after surgery. There are far too many patients, practically all those with massive and semimassive keloids, who have fallen onto the same path, which started with surgery to remove a small keloid lesion from their neck or another area of their skin.
Limited Role of surgery
Surgery, using a scalpel or a laser device, should never be used to remove early-stage, nodular, multi-nodular, or even semimassive tumoral neck keloids. Surgery is a known triggering factor in the formation of much larger neck keloids.
Surgery may only be considered in cases of massive neck keloids and only performed in coordination with a specialist physician who is familiar with keloid disorder and can administer proper adjuvant medical treatments, including ILC, in an attempt to prevent post-operative recurrence.
When contemplating surgery for patients with massive keloids, one has to be reminded that the lesion that is to be removed was most likely triggered by previous surgical removal of a smaller lesion.
Case Study 6
A 37-year-old African American male presented to the author in November 2015 seeking treatment for recurrent neck keloids (Figure 24). His struggles with keloid disorder started eight years earlier when he noticed small keloids on his neck. Subsequently, much like the patient presented in case study 5, this patient had also been treated with ILT and two rounds of surgery, each time followed by ILT. His keloids regrew after each surgery. Thereafter, he simply refused undergoing another surgery.
After much consideration, and with the limitations imposed by his work and his work schedule, he was started on ILC treatment with minimal response. In September 2017, almost two years after his initial presentation, he was referred for debulking surgery with the intention of aggressive post-operative adjuvant medical treatments. Figure 25 depicts the status of his neck keloids as of October 2018, approximately one year after the debulking surgery. Since his last surgery, he has been treated with ILT and ILC once every 6-8 weeks. The tumoral keloid on the left side of his face was not removed surgically due to technical issues related to approximating of the edges of the surgical wound. The patient’s work schedule has not allowed for cryotherapy to this lesion.

Figure 24. Case Study 6, Recurrent keloids along the surgical excision lines.

Figure 25. Case Study 6, one year after surgical removal of the tumoral keloids with continued post-operative adjuvant treatments with ILC and ILT.
References
- Tirgan, MH. Neck keloids: evaluation of risk factors and recommendation for keloid staging system, F1000 Research, June 28, 2016
- Tirgan, MH. Massive ear keloids: Natural history, evaluation of risk factors and recommendation for preventive measures – A retrospective case series, F1000 Research, October 13, 2016
- Miyahara H, Sato T, Yoshino K. Radiation-induced cancers of the head and neck region. Acta Otolaryngol Suppl. 1998;533:60-4
- Ron E. Cancer risks from medical radiation. Health Phys. 2003 Jul;85(1):47-59.
- Tirgan, MH. Laser Treatment of Keloid Lesions, Efficacy and Side Effects, Results of an on-line survey. Abstract – 2nd International Keloid Symposium, Rome, Italy June 7-8 2018. Full manuscript in press.
- Boomsma MJ, et.al. A Prospective Cohort Study on Radiation-induced Hypothyroidism: Development of an NTCP Model. Int J Radiat Oncol Biol Phys. 2012 Nov 1;84(3):e351-6.
- Nachalon Y, Katz O, Alkan U, Shvero J, Popovtzer A. Radiation-Induced Thyroid Cancer: Gender-Related Disease Characteristics and Survival. Ann Otol Rhinol Laryngol. 2016 Mar;125(3):242-6.