
Table 1. Distribution of keloid lesions among a cohort of 1088 patients.

Table 2. Demographics of patients and morphology of CSUA keloids.
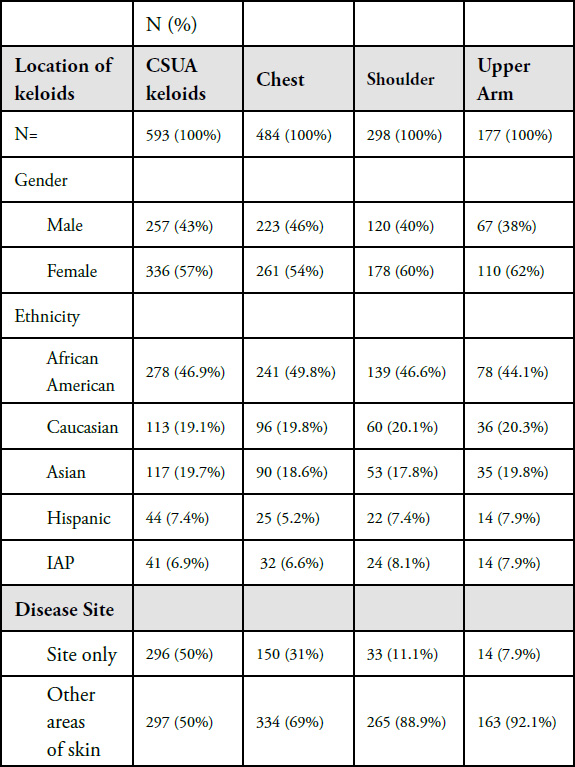

Figure 1. Early-stage papular chest keloid in a 22-year-old Asian female with a three-year history of keloid disorder.

Figure 2. A 27-year-old Caucasian male with a single anterior keloid papule present for two years.

Figure 3. Early-stage keloid papules in a 28-year-old Caucasian female with an eight-year history of keloid disorder involving her chest and shoulders. Note the presence of two midline keloid papules.

Figure 4. Linear chest keloid in a 53-year-old Caucasian female.

Figure 5. Two linear chest keloids in a 51-year-old Hispanic male.

Figure 6. Anterior chest keloid nodule in a 15-year-old African-American male. Note the sharp and clear circumferential border of this keloid.

Figure 7. A 25-year-old Asian female who presented with multiple facial and several papular chest keloids (June 2015).

Figure 8. The same patient, February 2016. Note that within the span of eight months the two medial keloid papules have grown in size and are growing towards each other.

Figure 9. The same patient, May 2016. Note that in span of one year since the initial presentation, the two medial papules have grown in size and merged to form a linear keloid. The lateral lesions have not merged.

Figure 10. The same patient in August 2018. Note that in a span of five months since initiation of treatment with ILC, the linear keloid remains active and exhibiting resistance to treatment, yet the two lateral papular lesions have responded to treatment and have almost completely regressed.

Figure 11. The same patient, December 2018. Note that in span of two and a half years, after several ILC treatments, the linear keloid still remains active and somewhat resistant to treatment, yet the two lateral papular lesions have completely regressed. The hyperpigmentation around the linear keloid is an expected reaction to the repeated ILC injections.

Figure 12. Previously untreated solitary anterior chest keloid in a 20-year-old Caucasian female.

Figure 13. The same patient after receiving three doses of ILT. Note the total flattening of the keloid two months after initiation of treatment.

Figure 14. Solitary anterior chest keloid in a 26-year-old male. Note the inflammatory margin of this lesion.

Figure 15. The same patient after receiving five cycles of ILT and contact cryotherapy. Note the total flattening of the keloid one year after initiation of the treatment.

Figure 16. Initial presentation of a 20-year-old Caucasian female with a two-year history of struggling with chest keloids (May 2012). Note the inflammatory reaction around the margins of all three lesions.

Figure 17. The same patient presented four months later (September 2012). Note the increased erythema and minor progression of the two adjacent lesions.

Figure 18. The same patient immediately after application of contact cryotherapy (September 2012). Frozen tissue appears white in color.

Figure 19. The same patient two months after treatment with contact cryotherapy (November 2012).

Figure 20. The same patient after three cycles of treatment (January 2013). Note near total ablation of the two merging lesions and reduction in the mass of the larger lesion.

Figure 21. The same patient after five cycles of treatment (June 2013). Note near total ablation of the two merging lesions but persistence of the larger lesion.

Figure 22. The same patient, five years after initial presentation (December 2017). Note the complete regression of the two merging lesions that were treated with ILT and cryotherapy in 2012-2013. The larger lesion is still present and slightly larger compared with the initial presentation in 2012.

Figure 23. The same patient after two doses of IL-VCR (December 2018). Note the significant reduction in the bulk and mass of the large lesion.

Figure 24. Untreated thick linear anterior chest keloid in a 39-year-old African-American female.

Figure 25. Thick linear anterior chest keloid in a young Caucasian female. Note the inflammatory border around the keloid.

Figure 26. Thick linear/nodular anterior chest keloid in a 36-yearold African-American female who has been struggling with keloid disorder since she was 13 years old.

Figure 27. Thick linear keloids of the anterior chest in a 38-year-old Indian female who has struggled with keloid disorder since she was 27.

Figure 28. Multiple thick linear anterior chest keloids in a 24-yearold Indian female who has struggled with keloids for three years.

Figure 29. Multiple thick linear and papular keloids of chest in a young Indian male.

Figure 30. A 29-year-old African-American male who presented with a three centimeter, previously untreated anterior chest wall keloid (April 5, 2014).

Figure 31. The same patient after receiving two cycles of contact cryotherapy (October 2014).

Figure 32. The same patient after three IL-CVR injections (March 2015).

Figure 33. The same patient four years after initial presentation (July 2018). Patient returned for treatment of the linear recurrence on the upper edge of the keloid. The linear lesion was injected with 2 micrograms of vincristine.

Figure 34. A 27-year-old Caucasian female with a ten-year history of widespread chest keloids. Note the multifocality of the keloids, merger and formation of keloidal patches, and inflammatory reaction around the larger lesions.

Figure 35. Multiple keloidal patches in a 28-year-old African-American female with a ten-year history of keloid disorder.

Figure 36. A 16-year old Caucasian male with a four-year history of widespread chest keloids triggered by acne. Note the merger and formation of the keloidal patch and the inflammatory reaction around most keloid lesions.

Figure 37. Widespread anterior chest keloids in a 29-year-old Caucasian male with a twelve-year history of keloid disorder.

Figure 38. Solitary tumoral anterior chest keloid in a young African-American female.

Figure 39. Thick keloidal tumor of anterior chest in a 34-yearold Hispanic female with an eleven-year history of keloid disorder involving her chest and shoulders. Note the formation of an earlystage linear keloid lesion in the left lateral margin of the main keloid.

Figure 40. A 37-year-old African-American female with a fouryear history of anterior chest keloids. She developed three distinct keloids in close proximity to each other.

Figure 41. A 28-year-old African-American female with a tenyear history of struggling with ear, chest, and pubic keloids. Note the two distinct anterior chest keloids in close proximity to each other.

Figure 42. A butterfly-shaped tumoral central chest keloid lesion in a 30-year-old African-American female with an eight-year history of struggling with keloid disorder.

Figure 43. A painful, butterfly-shaped tumoral central chest keloid in a 30-year-old Asian female with an eight-year history of struggling with the keloid shown here. Note the multifocality of the keloid lesions and the inflammatory skin reaction at the lateral margins of the large keloid. Central chest keloids of this magnitude are almost always pruritic, tender, and painful to the gentlest touch.

Figure 44. An irregularly shaped anterior chest tumoral keloid in a 42-year-old Middle Eastern female. This keloid first appeared as a small papule approximately twelve years earlier.

Figure 45. Large tumoral anterior chest keloid along with a smaller keloid in a 30-year-old female with an eleven-year history of struggling with chest keloid. Note the presence of intense inflammatory lateral margins.

Figure 46. Large tumoral chest keloids at presentation (November 12, 2013).

Figure 47. The same patient, two weeks after treatment with IL-VCR. Note reduction in the keloid’s mass and thickness (November 26, 2013).

Figure 48. The same patient, four weeks after initial presentation, having received two courses of treatment with IL-VCR. Note further redction in the keloid’s mass (December 12, 2013).

Figure 49. The same patient, two months after initial presentation, having received three treatments with IL-VCR. Note the further reduction in the keloid’s mass (January 7, 2014).

Figure 50. The same patient, two years after last treatment with IL-VCR. There was some regrowth of the keloid, yet the mass of keloid had remained smaller compared with the patient’s initial presentation (January 2016).

Figure 51. The same patient, immediately after application of contact cryotherapy (January 2016).

Figure 52. The same patient, four months after application of contact cryotherapy (May 2016). Note the reduction in the keloid’s mass.

Figure 53. The same patient, ten months after application of one cycle of contact cryotherapy and two treatments with IL-VCR (October 6, 2016). Note the further reduction in the keloid’s mass.

Figure 54. The same patient, after application of several cycles of contact cryotherapy and IL-VCR (March 1, 2018). Note the near flattening of the keloid. The cryotherapy’s induced loss of pigment is camouflaged with makeup. Although the results achieved are not ideal, they are significantly better than exposing this young patient to the risks associated with surgery and adjuvant radiation therapy.

Figure 55. An 18-year-old Caucasian female with a two-year history of DWACK syndrome presenting with multiple papular keloids of the anterior chest and both shoulders (May 2014).

Figure 56. An18-year-old Caucasian male with a two-year history of DWACK syndrome, presenting with widespread anterior chest and shoulder keloids, triggered by acne that was treated with isotretinoin.

Figure 57. A 22-year-old Caucasian male with only a one-year history of DWACK syndrome, triggered by acne and presenting with widespread chest and shoulder keloids. Note that the neck area skin is spared from the keloid process.

Figure 58. Superficially spreading anterior chest keloids in a 46-year-old African-American female with a six-year history of keloid disorder with a natural progression of the disease.

Figure 59. Locally advanced anterior chest keloid in a 55-year-old Caucasian female who has been struggleing with progressive anterior chest keloid since she was eleven years old. Note the presence of a fistula in the upper part of this keloid. Frequent deep infections are common complcations seen in patients with such thick aterior chest keloids.

Figure 60. A 29-year-old female with extensive keloid involvement of anterior chest area. This patients first keloids started in her chest at the age of 14. Note the presence of numerous keloid lesions that are in various stages of development, including newly developed papules. Progression of the disease in this patient has been autonomous. She denied having had any prior surgeries on her chest.

Figure 61. A 42-year-old African-American female presented with a thick linear incisional keloid six months after sternotomy.

Figure 62. A 75-year-old Caucasian male presented 15 years after a sternotomy with numerous painful and pruritic patches of keloid, mostly along the suture lines. Note the near absence of keloid formation along the midline incision. Most keloids are formed along the horizontal suture lines.

Figure 63. A 64-year-old Caucasian male who presented 14 years after a sternotomy with several pruritic and painful keloid patches mostly located along the suture lines, complicated with frequent infections and purulent discharge.

Figure 64. Keloid nodule with intense inflammatory borders in a 31-year-old Caucasian male. This keloid first started as a papule two years prior to this presentation. Keloid removal surgery was performed one year prior to this presentation. Unfortunately, there was a rapid recurrence after surgery.

Figure 65. A 31-year-old Hispanic female (October 2014) with a tumoral anterior chest keloid. Note the presence of inflammatory reaction around the margin of the main keloid and multifocal disease with two papular keloids in the immediate vicinity of the main lesion.

Figure 66. The same patient after recovery from three cycles of ILT and cryotherapy (July 2015). Note the thinning of the main keloid along with near-total flattening of the two keloid papules present at presentation.

Figure 67. The same patient after surgery and radiation therapy. Note the recurrent disease along the surgical incision line ( October 2017). Also, note that the small keloid papule previously present under the main keloid lesion, the one treated with ILT and cryotherapy, remained in remission with three years of follow up.

Figure 68. A 30-year-old African-American female with recurrent chest keloid after surgical removal of a small central chest keloid. Note the multifocality of the disease process.

Figure 69. Post-operative recurrent tumoral chest keloid in a 60-year-old African-American female.

Figure 70. Post-operative recurrent tumoral chest keloid in a 36-year-old Caucasian male with an 18-year history of struggling with this instant chest keloid, with four failed attempts at surgery and several ILT injections.

Figure 71. A 40-year-old African-American female with multifocal anterior chest keloids and recurrent disease after surgical removal of the keloid in her upper chest area.

Figure 72. A 26-year-old Caucasian female with extremely painful central chest keloids that developed shortly after surgical removal of two small keloids.

Figure 73. A 39-year-old African-American female with multifocal anterior chest keloids and recurrent disease after two surgical attempts and adjuvant radiation therapy.

Figure 74. A 27-year-old African-American female with recurrent disease after surgical removal of two anterior chest keloids.

Figure 75. A 42-year-old African-American male with recurrent anterior chest keloid after surgical removal of an upper chest keloid.

Figure 76. A 51-year-old African-American male with a ten-year history of keloid disorder. A smaller chest keloid was removed surgically six years earlier, which led to the formation of a large tumoral central chest keloid that has been constantly growing in size and complicated with frequent infections.

Figure 77. A 37-year-old African-American male with semimassive chest keloid that grew after the surgical removal of a smaller keloid. Note the presence of a non-healed draining fistula in the lower central part of this keloid. Frequent infections are among the most common commplications of massive chest keloids.

Figure 78. A 49-year-old African-American female with asemimassive chest keloid that grew after surgical removal of a smaller keloid.

Figure 79. Massive central chest keloid in a 38-year-old African- American female who had previously undergone surgery to remove a small central chest keloid.

Figure 80. Massive central chest keloid in a 57-year-old African- American female who had previously undergone surgery to remove a much smaller central chest keloid.

Figure 81. A 43-year-old Asian male with recurrent chest keloid despite prior treatment with surgery and radiation therapy. The multifocality of the disease strongly argues against the benefit from surgery, with or without radiation.

Figure 82. Multiple recurrent chest and shoulder keloids in a 34-year-old African-American male who had previously undergone surgery to remove keloids in the small central chest, lower neck, and left shoulder.

Figure 83. Superficially spreading anterior chest keloid in a 37-year-old African-American male who had previously undergone surgery to remove a small central chest keloid.

Figure 84. A 55-year-old male with extensive superficially spreading of chest wall and shoulder keloids, previously treated with multiple surgeries and adjuvant ILT injections.

Figure 85. Post-operative recurrences in a 47-year-old male with extensive multifocal keloids since the age of 16. This patient had undergone surgery to remove several of his chest lesions followed with adjuvant ILT injections.

Figure 86. A 36-year-old old African-American female with massive neck and chest keloids. Note that her neck and chest keloids have merged, forming a very large, superficially-spreading keloid extending from her right ear to her neck, anterior chest, and left shoulder.

Figure 87. A 27-year-old African-American female with extensive superficially spreading chest wall keloid, previously treated with multiple surgeries and radiation therapy. Another example of how harmful and life-changing our treatments can be.

Figure 88. Multiple papular keloids of the anterior chest in an 18-year-old Caucasian female who has been struggling with keloid disorder for two years (May 2014).

Figure 89. The same patient, four years later (February 2018). She has not developed any new lesions and treated lesions appear to be much improved.

Figure 90. Two tumoral keloids of anterior chest wall in a 21-yearold African-American female (April 2014).

Figure 91. The same patient in April 2017, almost three years after her initial presentation. Note the significant growth and enlargement of the two anterior chest keloids present in 2014.

Figure 92. Anterior chest keloids in a 23-year-old Indian male (August 2016).

Figure 93. Close up view of the same lesions depicting response to the ongoing laser treatments. Several lesions appear to have diminished in size or totally flattened (August 2016).

Figure 94. The same patient in January 2019. Note the progression of the disease and the formation of new lesions in a span of two and one-half years.

Figure 95. Numerous anterior chest keloids in a 25-year-old African- American male who had undergone several surgeries and radiation therapy to remove several of his chest wall keloids (April 2014).

Figure 96. The same patient in August 2017. Note the significant progression of the disease in a span of three years.

Figure 97. The same patient in January 2019. Note the significant progression of the disease in span of four and one-half years.